
Case 4
- alocoordinator
- Feb 21, 2024
- 2 min read

"A 53-year-old male presented in the Radiation Oncology clinic with a complaint of hoarseness of voice for 6 months. On flexible fiber optic laryngoscopy (FODL), a lesion was identified on the left vocal cord. A biopsy sample was taken, which was consistent with squamous cell carcinoma. A CT scan revealed a lesion in the left vocal cord with bilateral cervical lymph nodes. On examination, the patient was grossly unremarkable, with no palpable cervical lymph nodes.
PET CT scan was done for staging workup due to involvement of primary echelons for laryngeal cancer, showing fluorodeoxyglucose (FDG) avid bilateral cervical lymph nodes. Considering nodal involvement despite the small size of the primary lesion (T1), the case was discussed with radiologists & concluded as suspicious of metastasis as the SUV for primary & nodes is in similar range. Therefore, the radiation plan was contoured to include the primary glottis lesion and bilateral cervical lymph nodes.
The case was presented in a Peer Review Meeting, and it was recommended to obtain a biopsy of the cervical lymph nodes as chances of T1 glottis to metastasize to lymph nodes are less. (<5%). Fine-needle aspiration cytology (FNAC) was performed, which was negative for malignancy. Subsequently, the target volume for radiation therapy was reviewed, and it was contoured for the glottis only, following recommended guidelines for T1 glottic cancer."
IMAGING
· A CT scan revealed a lesion in the left vocal cord measuring 1.1 x 0.5 cm. Multiple enlarged lymph nodes were observed in the bilateral submandibular gland region, with the largest one on the left side measuring 1.6 cm.
· A PET/CT scan showed mildly fluorodeoxyglucose (FDG) avid asymmetry involving the left vocal cord, measuring 1.5 x 0.5 cm, with a standardized uptake value (SUV) of 2.7. Additionally, FDG avid bilateral cervical lymph nodes were identified, with the largest measuring 1.8 x 0.9 cm (SUV 2.4) on the left side
LEARNING POINTS
·Correlating the radiological findings with the natural history of the tumor is essential, considering that it is less likely for T1 glottis tumors to metastasize to cervical lymph nodes.
·Confirming any discrepancy with the biopsy is crucial to rule out other causes of FDG avid lymph nodes.
·Avoiding overtreatment is important, and sparing neck nodal levels would be beneficial, especially in the event of re-irradiation if such a scenario develops.
·This case highlights the Importance of intra-departmental peer review meeting, to Review all radical treatment volumes before proceedings for planning could make a huge impact in decision making which will ultimately result in better outcomes for patients
·It also enlightens the role of Peer Review in reporting as well as for all radiology & functional imaging.



FIGURE 1
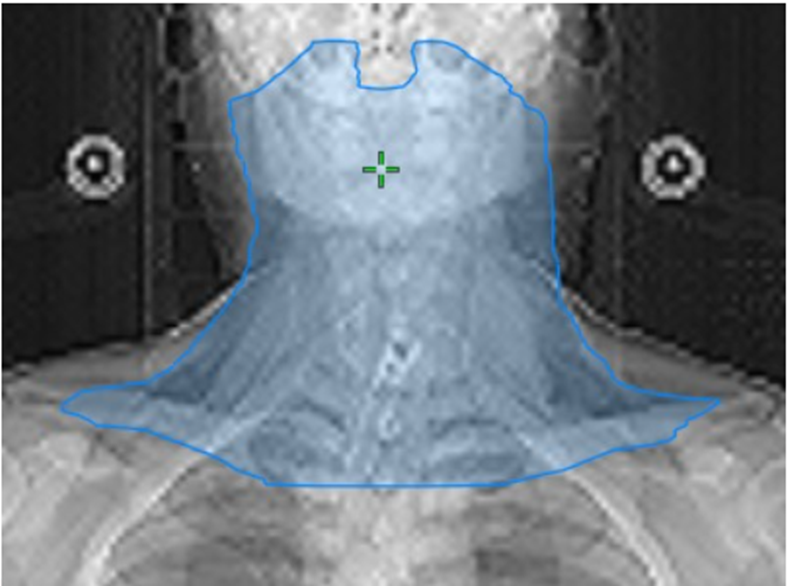
Target volume Delineation for Node positive Glottic Ca

Target volume Delineation for T1 Glottic Ca



Comments